Total Knee Arthroplasty

Total Knee Replacement (TKR) or Total Knee Arthroplasty (TKA), is the most common joint replacement surgery performed in Canada today. In its modern iteration, the TKA was developed over 40 years ago, by Drs. Insall, Burstein and Ranawat at the Hospital for Special Surgery – where Dr. Rodriguez-Elizalde did his fellowship training.
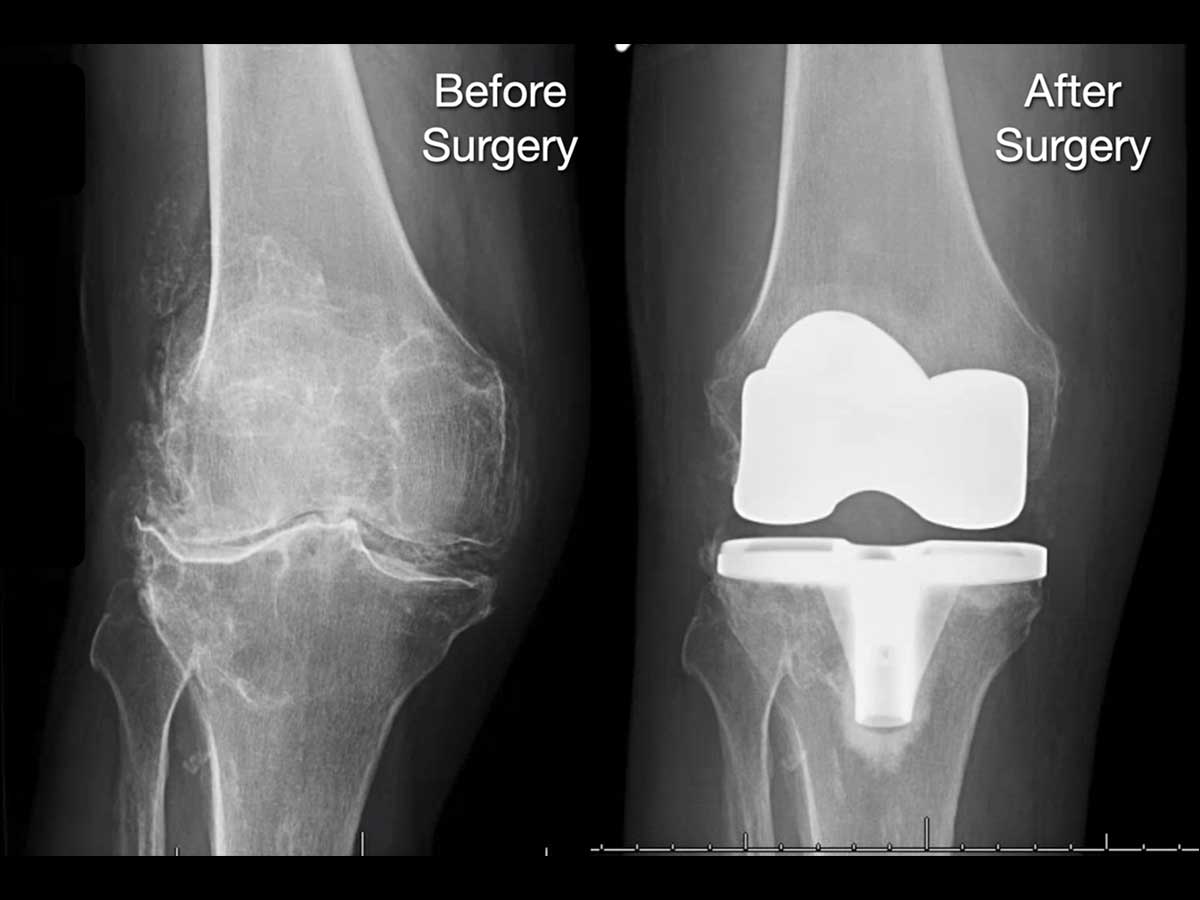
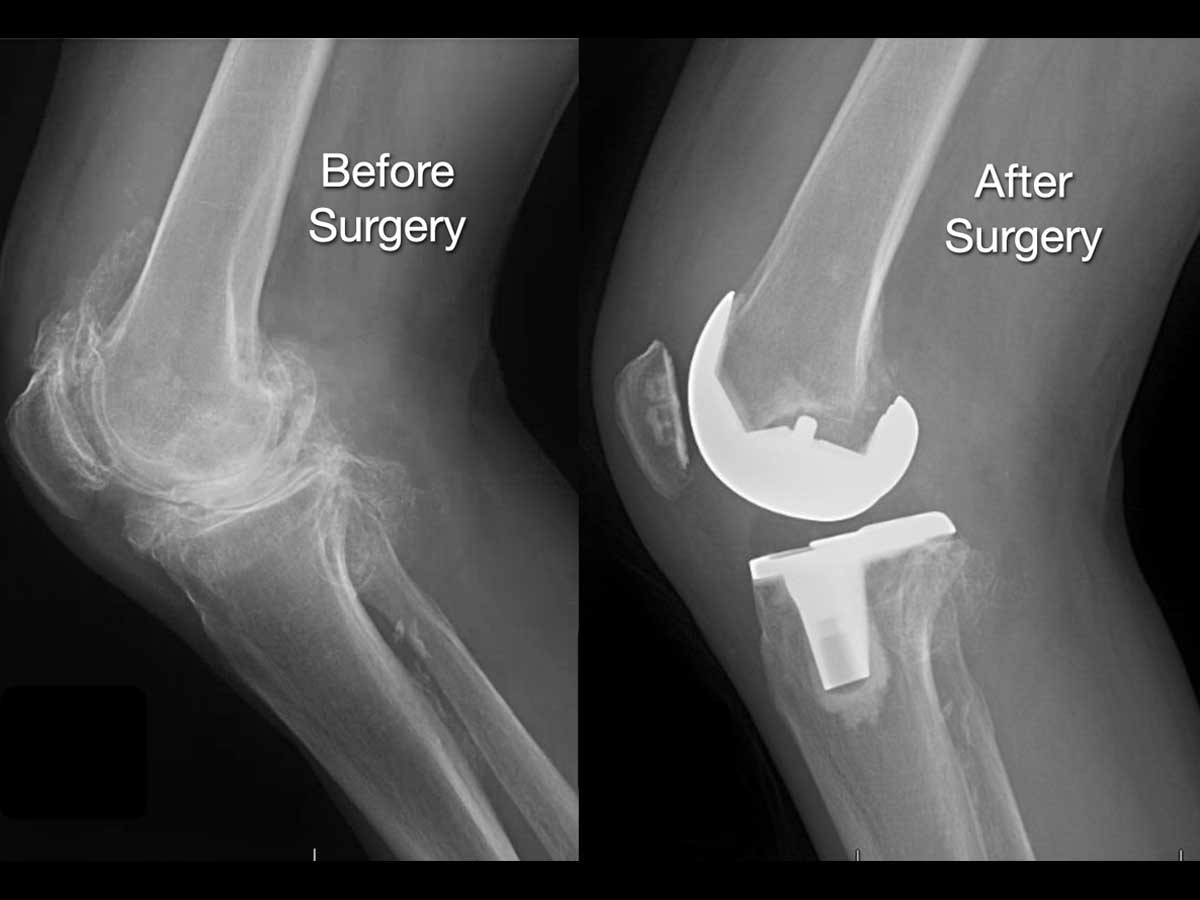
Total Knee Arthroplasty is reserved for definitive management of arthritic or post-traumatic changes in the knee. Once the smooth articular surface (cartilage) of the knee is worn out, and pain medication, injections and physical therapy can’t help, surgery may be the answer. It is used primarily to alleviate pain, gain function and restore alignment in the knee.
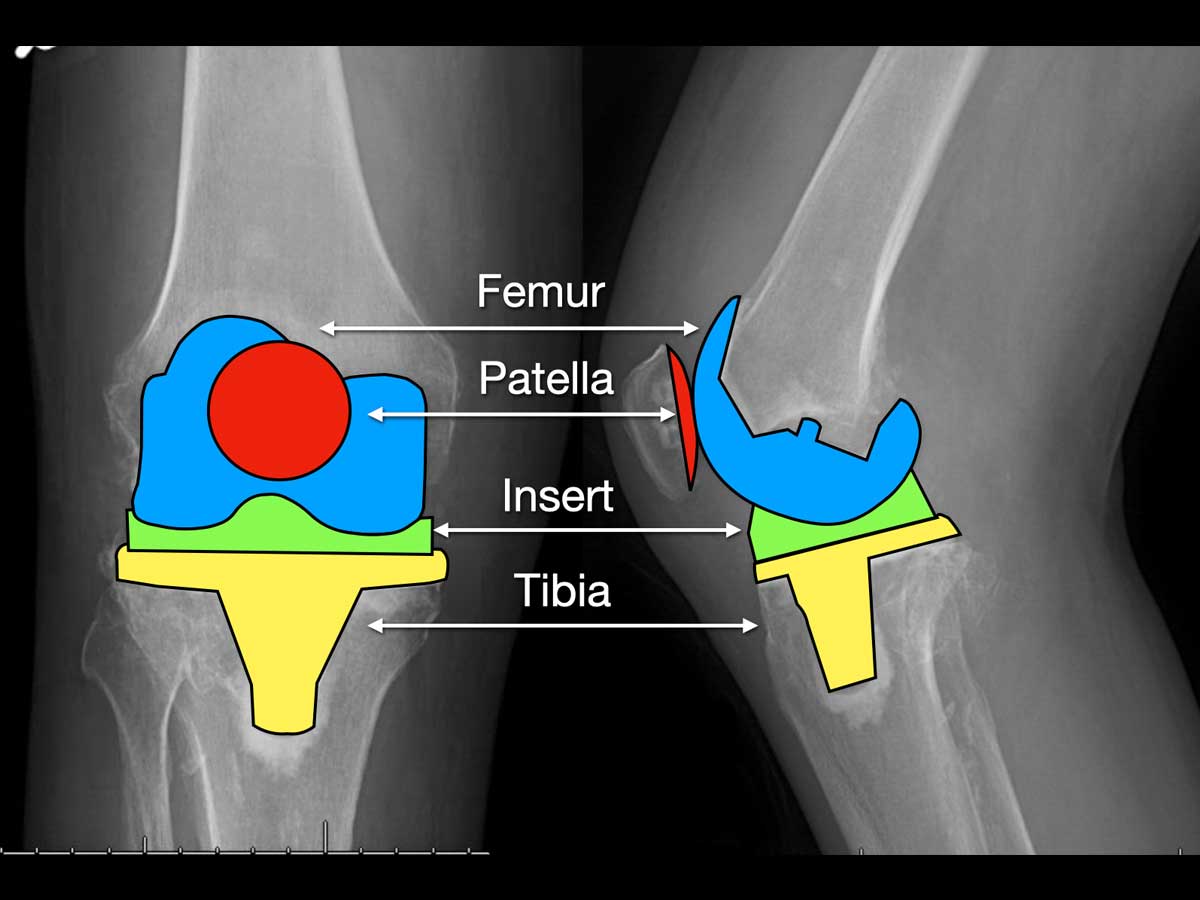
Total Knee Arthroplasty involves the surgical replacement of the articular (joint) surfaces
of the knee including the:
1. Bottom part of the Femur (thigh bone), by a cobalt-chromium alloy cap
2. Top part of the Tibia (shin bone), by a titanium metal alloy plate
3. Undersurface of the Patella (knee cap), by a plastic polyethylene cap
4. Between the metal pieces, a plastic articular surface is inserted
- FAQ
What is my expected recovery?
You will spend two nights in hospital after your procedure. After you wake up the day of your surgery, you will start to mobilize with a physiotherapist at the side of the bed, and practice transfers to a chair. You can put your full weight on your operated leg, but have to wait until the nerve blocks used for anesthesia wear off, before moving without a knee brace.
Physiotherapy is important in Total Knee Replacement surgery. The more you move, and push the progression of your range of motion, the better the outcome.
Once safe and comfortable, you will be discharged home with a prescription for painkillers, blood thinners and anti-Inflammatories. You will see Dr. Rodriguez-Elizalde 10-14 days after surgery in the fracture clinic for examine the wound and to check your progress.
The next visit is at 6 weeks, and involves a clinical check and x-rays.
Overall, in terms of recovery, you will likely need a walker or cane for the first 4-6 weeks. A rough estimate of a timeline is a 50% improvement at 6 weeks, and 80% at 12 weeks. The last bit of recovery is mainly endurance training to help combat fatigue and stiffness. This can take up to a year to improve. The most common complaints are stiffness, ache and swelling in the front of the knee. Your deep “arthritic joint” pain should be gone the minute you wake up from surgery, but post-surgical pain in Total Knee Replacement surgery can be significant.
The most important thing to remember is that recovery varies for everyone. Dr. Rodriguez-Elizalde prefers to monitor your progression vs an absolute timeline. As long as you continue to improve week to week, you are doing well.
Back to work?
This question varies a lot on what you do, and any accommodations that can be made for you at work and at home. Most importantly is depends on you – your expectations, drive and recovery are all variable. Most “desk” type jobs can be resumed around 8-12 weeks later, sooner in some cases. Most physical jobs will need a stronger recovery, typically 3-4 months.
Driving?
You may drive when:
1) You are no longer taking narcotic pain medication
2) You have full power and function to engage in emergency braking
of your car if necessary.
This usually takes a minimum of 6 weeks.
What activities can I do?
After your knee replacement has healed, you may return to all day-to day activities. In terms of recreational activities, patients may return to skating, skiing, light weight lifting, swimming, bowling, golfing, tennis, squash, biking and use of an elliptical trainer. The only restriction is high impact jumping and running type activities. This is more Dr. Rodriguez-Elizalde’s personal preference, as there is no direct medical evidence that those activities cause early failure. That being said, running and jumping cause very high joint reactive forces through the hip, and thus are thought to lead to earlier implant failure.
Kneeling can be tolerated in about half of patients post Total Knee Replacement. The prosthesis is cemented in and can withstand kneeling, but the scar tissue that develops in a lot of patients makes it uncomfortable to knee.
Flying/Travel
Flying and long distance travel should ideally only be done 6 weeks after surgery. Short flights and travel can be undertaken after 7-10 days after surgery, but you should get up and move every hour, and will require a prescribed blood thinner.
The largest hindrance of travel is how you are feeling. You may still need a walker or cane to mobilize safely, and will be moving through crowded areas. Planes, buses and trains are cramped and sitting for long periods of time will cause stiffness and pain in the knee.
In summary, if you are able to delay your travel for the first 6 weeks, you will certainly enjoy your trip more. Short flights, and those necessary for returning home after surgery should not be done before 7 days, and will require a prescribed blood thinner.
Do I need Antibiotics Before a Dental Procedure?
No. This is different than Dr. Rodriguez-Elizalde’s previous recommendations where a dose of antibiotics was given prior to any dental procedure for life.
In reviewing the recent literature and position of the American Dental Association, the use of antibiotics prior to dental work is not necessary. http://www.ada.org/en/member-center/oral-health-topics/antibiotic-prophylaxis
There is no association of hip or knee infection with or without administration of antibiotics before dental work – so we have changed our policy and no longer require you take them.